The maximal voluntary ventilation (MVV) measurement is defined as the maximal volume of air that can be moved by voluntary effort in 1 minute. Subjects are instructed to breathe rapidly and deeply for 15 to 30 seconds, ventilatory volumes are recorded, and the maximal volume achieved over 15 consecutive seconds is expressed in liters per minute. Lung volumes are reported at the largest size possible within the chest and at body temperature (37° C) and standard pressure fully saturated with water vapor (760 mm Hg).
The observer should demonstrate the test; then the subject should choose his or her own respiratory rate and perform several practice runs. The respiratory frequency used in the MVV should be noted and recorded as a subscript (e.g., MVV90 or MVV110). Maximal levels are usually achieved between 70 and 120 breaths/min, but the choice of frequency does not greatly affect the test.
This test is heavily dependent on subject cooperation and effort. Loss of coordination of respiratory muscles, musculoskeletal disease of the chest wall, neurologic disease, and deconditioning from any chronic illness, as well as ventilatory defects, decrease MVV, so the test is nonspecific. The MVV is decreased in patients with airway obstruction, but less so with mild or moderate restrictive defects because rapid, shallow breathing can compensate effectively for the decreased lung volume.
Despite these caveats, MVV can be useful in special circumstances. It correlates well with subjective dyspnea and is useful in evaluating exercise tolerance. It appears to have prognostic value in preoperative evaluation, possibly because the extrapulmonary factors to which it is sensitive are also important for recovery from a surgical procedure. It also provides a measure of respiratory muscle endurance that may be important in the evaluation of respiratory muscle fatigue, whether from obstructive or restrictive ventilatory defects or from specific neuromuscular diseases. In myasthenia gravis, for example, the patient can often produce maximal efforts for a short time, so that FVC and maximal inspiratory and expiratory pressures are normal. However, the effort cannot be sustained, so the MVV or repeated FVC values decrease, even within 12 to 15 seconds. The respiratory crisis of myasthenia gravis may happen rapidly and lead to respiratory failure. As a result, some investigators have suggested that MVV should never be measured in patients with myasthenia gravis, except under carefully controlled circumstances when it may be useful in evaluating treatment.
Source: Warren M. Gold MD, Laura L. Koth MD, in Murray and Nadel's Textbook of Respiratory Medicine (Sixth Edition), 2016
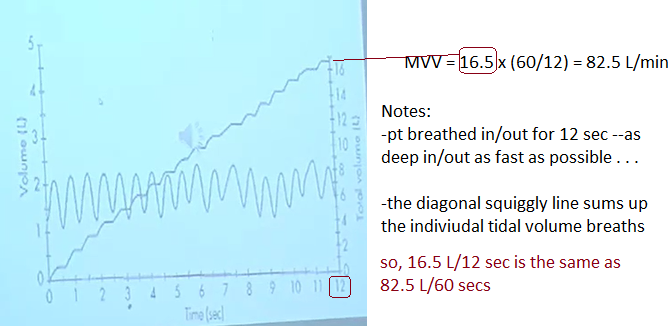
For 12 seconds, have pt breath in deeply & exhale, repeat vigorously. In a sense, MVV reflects the efficiency of lung recoil.
Maximal voluntary ventilation (MVV), also referred to as maximal breathing capacity (MBC), is defined as the maximum minute volume of ventilation that the subject can maintain for 12 s. In the normal subject MVV is about 15 to 20 times the resting minute volume.
The maximal voluntary ventilation (MVV) is the largest amount of air that a person can inhale and then exhale during a 12- to 15-s interval with maximal voluntary effort (Neder et al., 1999). This maneuver was used to provide information about the functioning of the inspiratory pump and chest wall and is used to evaluate maximum ventilatory capacity (Colwell and Bhatia, 2017) and respiratory muscle endurance, but the last ERS statement on respiratory muscle tests does not recommend its use for these purposes because mechanical aspects of the chest wall and lung tissue can affect the MVV value (Laveneziana et al., 2019). It is used for indirect calculation of the ventilatory reserve through a relationship with minute volume during a maximum exercise test (ATS/ACCP, 2003). The performance of this test can be modified by factors such as strength and endurance of the respiratory muscles and/or airways as well as chest wall biomechanics (Barreiro and Perillo, 2004; Pellegrino et al., 2005; Suh and Lee, 2017).
Subjects who have pulmonary disease will show decreased absolute values. MVV is usu normal in restrictive dz.
MVV = Total Volume x (60/12) = answer is in L/min
Normal male: 80 - 160 L/min
Normal female: 60 - 120 L/min
<75% normal = significant
-poor pt effort
-neuromuscular dz (GB, MG)
-obstructive airways: can't get air out
Want ~ 2 breaths per second of rapid in/out breathing. Want 90-100 breaths/min!
Each breath should ~ 50% of VC.
Sources:
https://www.frontiersin.org/articles/10.3389/fphys.2020.00537/full -- Maximal Voluntary Ventilation Should Not Be Estimated From the Forced Expiratory Volume in the First Second in Healthy People and COPD Patients
Video:
Broward College Respiratory Lecture 2017 on MVV, FRC, RV, DLCO