How are lung volume determination results interpreted in pulmonary function testing?
Ans:
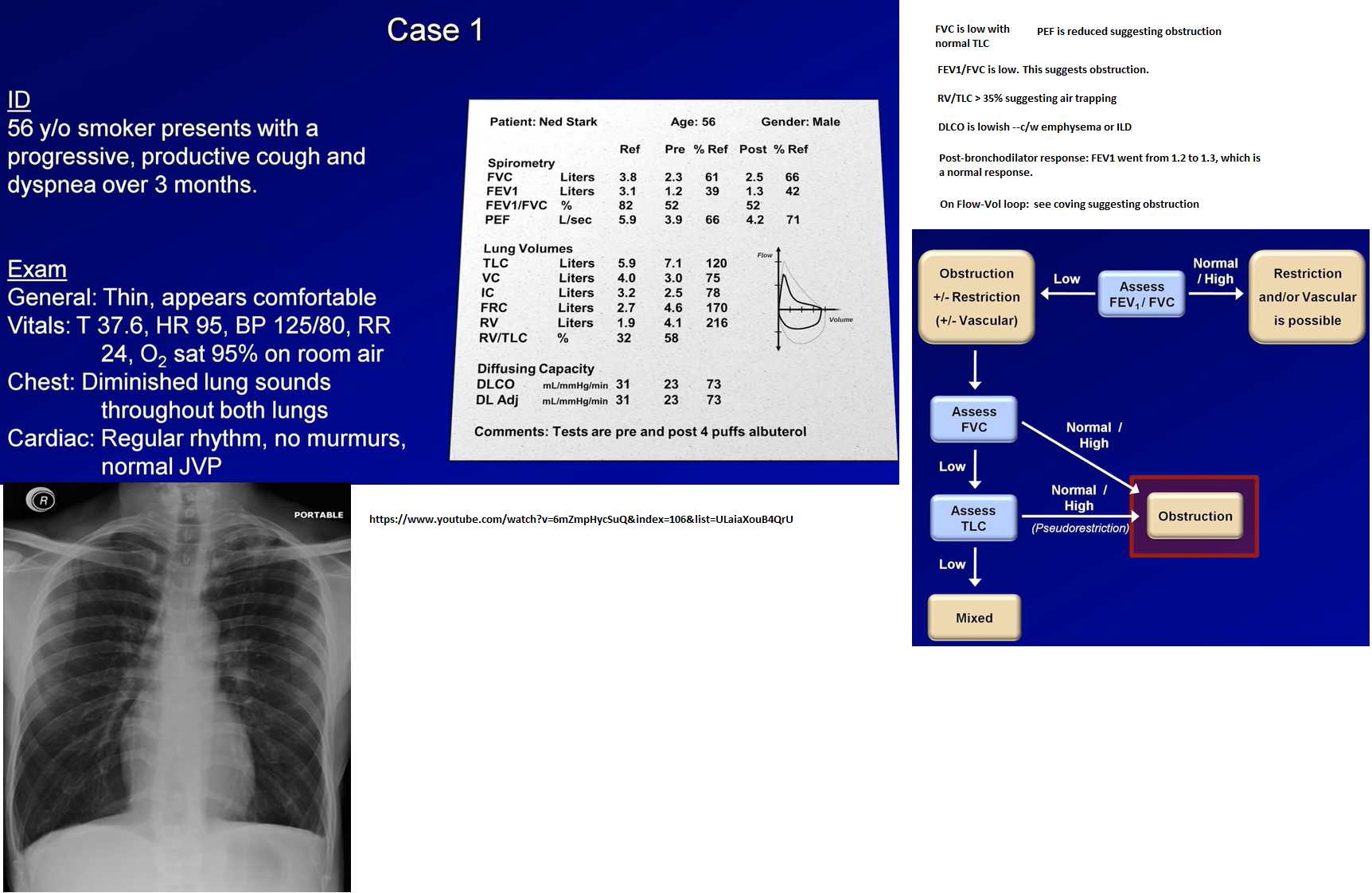
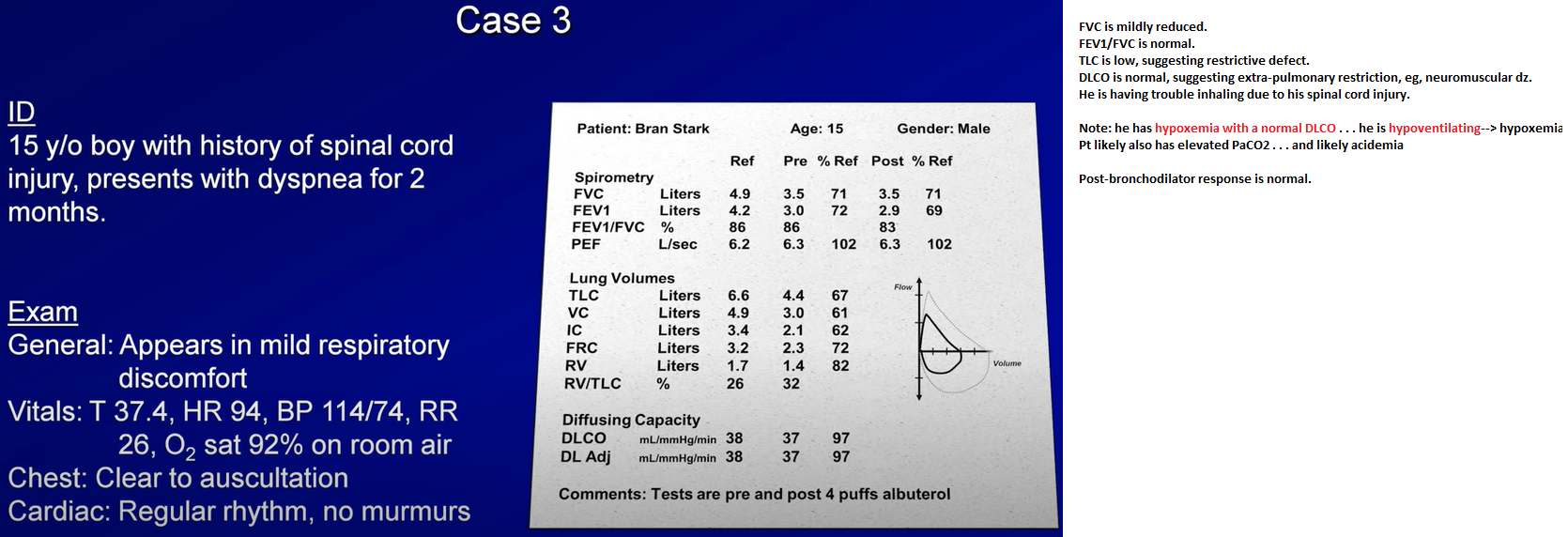
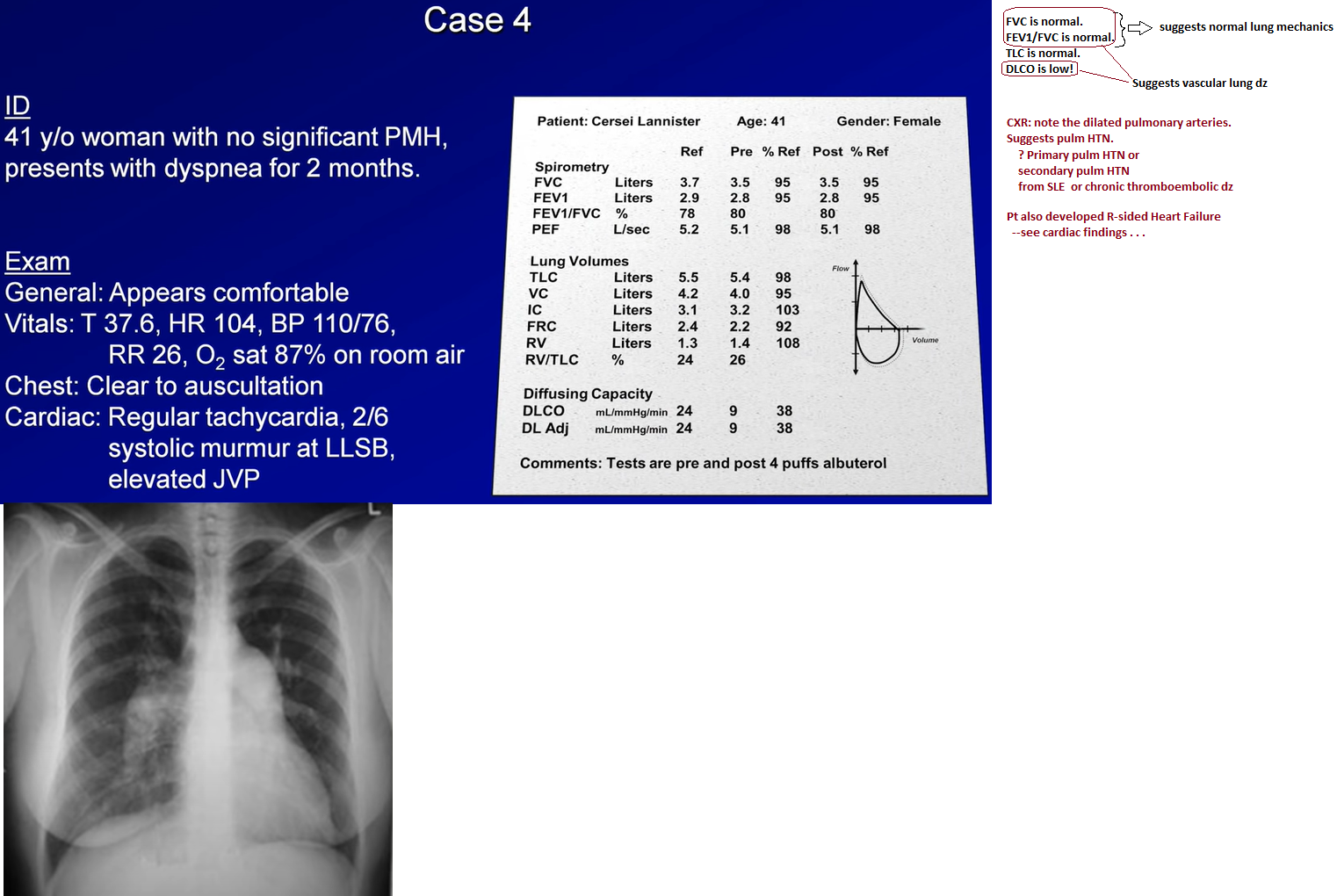
Obstructive lung diseases, particularly emphysema, result in an increase in the RV & RV-to-TLC ratio. In severe emphysema, particularly bullous emphysema, the TLC can show a marked increase. Bronchial spasm, airway inflammation, excessive secretions in the airway, & loss of lung elastic recoil increase airways resistance & result in an insidious progressive increase in the end-expiratory lung volume that results in chronic hyperinflation (elevated RV, TLC, and RV-to-TLC ratio). Other pulmonary causes of increased RV include pulmonary vascular congestion & mitral stenosis. Extrapulmonic causes of increased RV include expiratory muscle weakness as observed in spinal cord injuries & myopathies.
Increased body weight due to increased fat causes an increase in chest wall elastic recoil, which favors a lower end-expiratory lung volume, resulting in less hyperinflation for any degree of airflow obstruction.
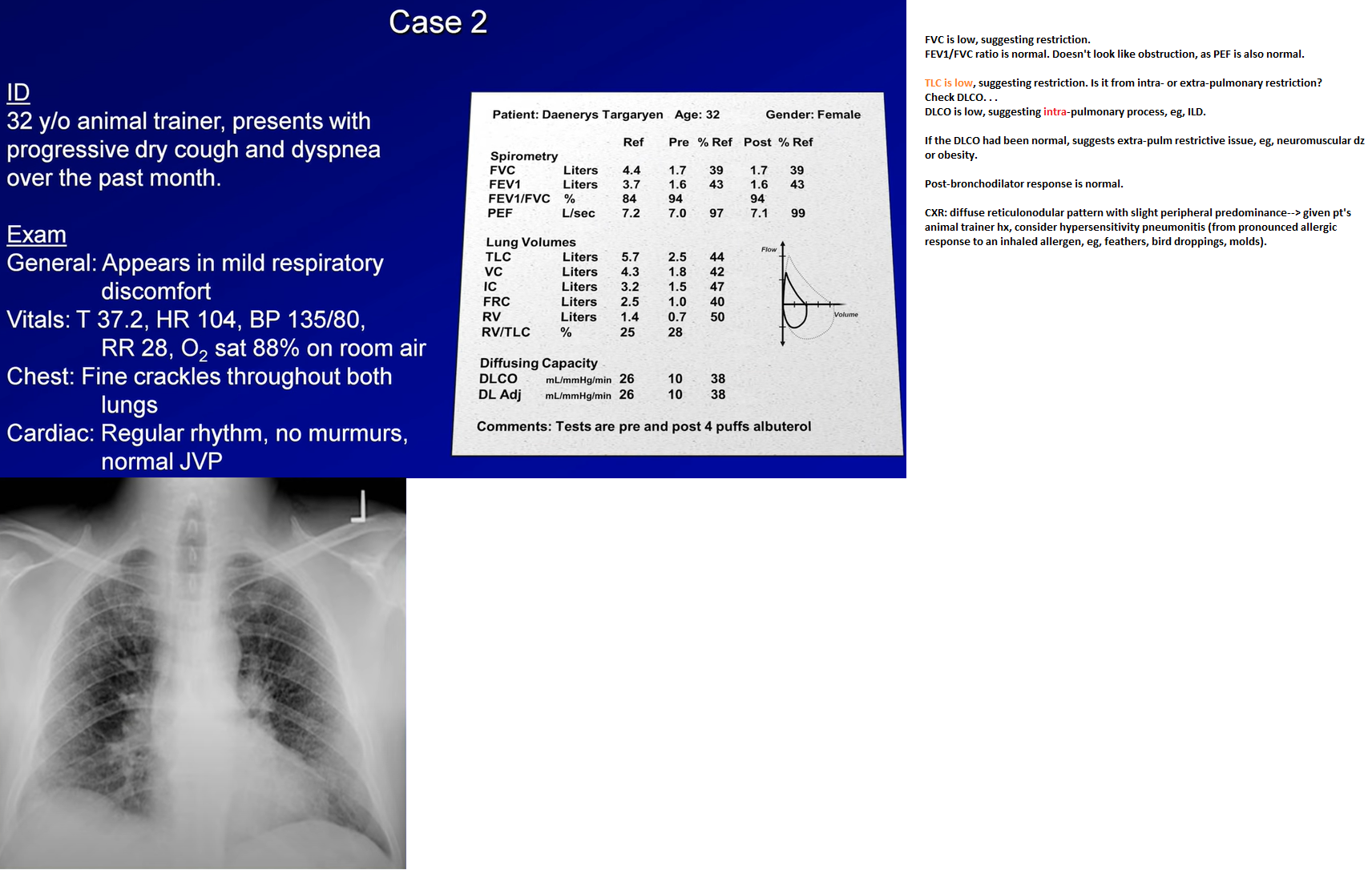
Lung volumes can confirm the presence of restriction when a reduced vital capacity is seen on spirometry. A reduced TLC is the hallmark of restrictive lung disease. An isolated reduction of the residual volume may be an early sign of restrictive lung disease. Pulmonary processes that can reduce the TLC include interstitial lung disease, atelectasis, pneumothorax, pneumonectomy, consolidation, edema, & fibrosis. Extrapulmonary causes of restriction include obesity, respiratory muscle weakness, thoracic deformities, & disease of the pleura.
Lung volume determinations are used in the evaluation of suspected restrictive lung disease and the evaluation of hyperinflation.
Source:
McCarthy K. Pulmonary Function testing. 2020. Medscape
https://emedicine.medscape.com/article/303239-overview#a2
Bates D, Mandel J. Pulmonary Function Tests. Hospital Medicine
*****
*****
*****
*****
Videos:
Pulmonary Function Tests (PFT): Lesson 5 - Summary and Practice Cases